

It sure does stop your heart. This summer I was selected to participate in the Stanford High School Summer College. This was a program that allowed high school students to take real undergraduate courses for the eight week summer quarter. Needless to say, starting on June 20, 2016, I was in for a ride.
I live in Novato, and Stanford is in Stanford (it is it's own municipality, with a post office and everything), which is near Palo Alto. Below I've attached a map just to give you an idea of my commute.
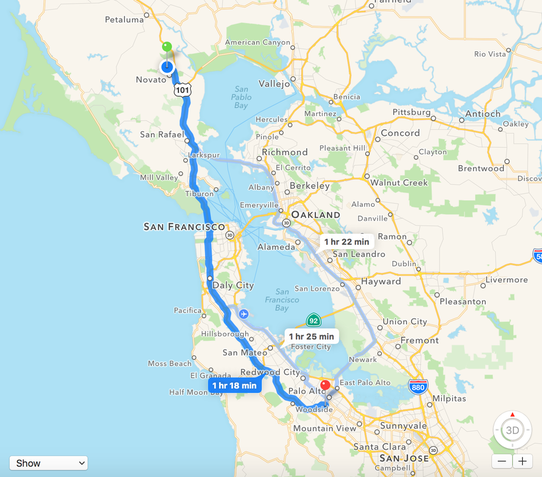
As you can see from the picture, it wasn't an easy haul. My dad would drive me in. After class, I would take Caltrain back to the city and walk two miles to his station (where he worked). Surprisingly, this was the easy way. Because I had basketball practice 5-7pm everyday and my dad couldn't leave work until 7pm, I had to find another way of commuting. The solution: take the ferry to the city, walk just under two miles to the Caltrain station, take Caltrain to Palo Alto, and take the free Marguerite Shuttle (my life saver) to campus. After class, I would race to make the 12:26pm shuttle on Line P and travel home by train, foot, and boat. It might sound intimidating at first, but I learned to love the commute. In the morning, I felt part of the rush. I learned how to grab a seat on the 7am ferry. I got to know a father and his daughter who traveled to the city together--work for him and pre-school for her. The train back home was in the middle of the day. Needless to say, I was one of twenty passengers. I got to know one of the Caltrain officers. She loved to hear about what I learned in class, and I was thrilled to talk about it. The commute itself was a great experience.

Now let's talk about the class itself--Abnormal Psychology. I will be honest that it wasn't my first choice, but by the end of the eight weeks, I was so thankful I took this class. I have always wanted to study how the body works, what allows us to live and thrive. However, I never asked, "What makes us think?" This summer I learned about the amazing, powerful (there are no words to describe it) brain. There are 100 billion neurons in the brain, each one firing signals. We can touch, we keep breathing, our hearts beat because of the brain. In this course specifically, I learned about what happens when something goes wrong in the brain. With great power comes great loss as well, and sadly, many people suffer from these losses.

If you take any Psychology course, you will run into the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). DSM is the official taxonomy of psychological disorders and their diagnostic criteria. DSM was created by the American Psychological Association with the help of clinicians and researchers. DSM is mostly used in research rather than clinical settings usually because there are certain biases amongst clinical psychologists, counselors, and psychiatrists. We can follow the evolution of societal norms by looking at past diagnoses. People thought there was something psychologically wrong with someone who behaved and thought differently. DSM-5 has worked to update and improve the diagnoses in the manual according to modern societal standards.
We started with the history behind the treatment of mental disorders, and unfortunately, it is not a pretty one. No one knew why people acted strange, so they would blame the person. They believed they either offended the gods or they were witches, torturing them and performing trepanations (drilling a hole in a person's skull to release the evil spirits). It was institutions like the Priory of St. Mary of Bethlehem, or "Bedlam", that improved the quality of care for the mentally ill, at least showing some compassion. However, patients were still on display, mocked and judged by the public. In more recent centuries, the Moral Treatment Movement swept across the United States and Europe. It was people like Dorothea Dix that created change. She saw how inmates and the mentally ill lived in prison when she taught Sunday school there. That experience drove her to speak to the people. Thanks to her, public mental hospitals erupted across the country. Not only did we learn about the past, but we examined the present. Psychological disorders are the most stigmatized treatments of the twenty-first century. As a class, we discovered the biggest obstacle to better treatment is the stigma behind mental disorders.
Next, we studied the different approaches that have been used to treat mental disorders. Some of the early biological approaches included Louis Pasteur's germ theory, insulin-induced comas, electroconvulsive therapy (ECT), and surgical lobotomies and lobectomies. Some of these techniques are still used today. For example, ECT still remains the most effective treatment for mental disorders, but now it's less painful and more humane (so not like what you would see in One Flew Over the Cuckoo's Nest).
After looking from a biological point of view, we stood from a psychoanalytic point of view. One of the most well-known theories is Sigmund Freud's Psychoanalytic Theory. To him, there were three parts of the mind: the id, the ego, and the superego. The id was one's basic instinctive drive while the superego was one's conscience, or sense of morality. The ego was one's perception of reality, or the mediator between the id and superego. Because of this, we had unconscious conflicts between the id and the superego. Freud further broke down eight defense mechanisms: repression, denial, projection, displacement, reaction formation, regression, rationalization, and sublimation. So how could Freud's theory be used to treat mental disorders?
After looking from a biological point of view, we stood from a psychoanalytic point of view. One of the most well-known theories is Sigmund Freud's Psychoanalytic Theory. To him, there were three parts of the mind: the id, the ego, and the superego. The id was one's basic instinctive drive while the superego was one's conscience, or sense of morality. The ego was one's perception of reality, or the mediator between the id and superego. Because of this, we had unconscious conflicts between the id and the superego. Freud further broke down eight defense mechanisms: repression, denial, projection, displacement, reaction formation, regression, rationalization, and sublimation. So how could Freud's theory be used to treat mental disorders?

Franz Anton Mesmer and Jean-Martin Charcot are the minds behind hypnotism. Both were two pre-Freudian psychiatrists practicing medicine. They believed through hypnosis, they could reduce the caliber of hysteria present in a patient. A Viennese physician named Josef Breuer offered another approach: the cathartic method. His most famous case was the case of Anna O. She had sight and hearing problems, partial paralysis, speech deficits, and "dream" states. By forcing her to relive emotional experiences and express her feelings from that time, he reported he permanently cured her. However, this was only partially true. She was only cured temporarily, and she still needed morphine to treat her hysterical problems. Three major techniques of psychoanalysis include free association, interpretation, and analysis of transference. While free association allowed a person to spill out information without censoring it, interpretation and analysis of transference required the psychologist to play a role, either as the interpreter or the target of the patient's bad feelings.
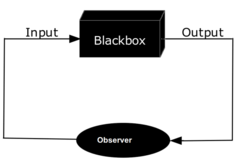
Although psychoanalytic theories dominated for some time, others like the psychodynamic theory and behaviorism developed. Carl Jung's and Alfred Adler's psychodynamic theory added to Freud's theories the concept of the collective unconscious, personality traits, and individual fulfillment to the social good. While psychodynamics were similar to psychoanalysis, behaviorism went the opposite direction. Instead of focusing on all the thoughts that come in between (the black box), they observed the cause and effect, the input and the output. John Watson was the man who aided the shift to behaviorism, but Ivan Pavlov and B.F. Skinner themselves were instrumental to the approach.
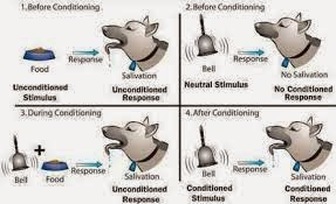
Many have heard of Pavlov's dogs, but do they know what he was researching? Pavlov discovered that when ringing a bell before bringing out food, the dogs will associate the bell with food. Therefore, at the ring of a bell, the dogs would salivate. This was known as classical conditioning. When I hear the song "300 Violin Orchestra", I immediately become anxious because it is the song my team runs out to for basketball games. I associate the song with high pressure games, and I feel that same anxiety when the song plays. In fact, psychologists use classical conditioning to treatment disorders like Obsessive Compulsive Disorder through a technique known as Systemic Desensitization. By exposing patients to certain conditions, they learn to associate those tasks with non-threatening and low stress experiences.
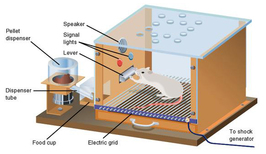
Skinner's Box is proof of operant conditioning. In this box, a rat learned to pull a lever in order to receive a treat. Because he associated something by doing something, it was classified as operant conditioning. On our test, our teacher used "Pokemon Go" as an example of operant conditioning. You wanted to keep playing because you were rewarded points. This is true with most games.
Alfred Bandura, who did research at Stanford (pretty cool), used Baby Alfred to explain the approach of modeling. First, they instilled a fear of rats into baby Alfred. Then by showing the baby people who interacted positively with the rat, Baby Alfred learned to not fear rats.
Next came the cognitive approach to psychological disorders. Albert Ellis developed the rational-emotive behavior therapy (REBT). Ellis prompted that by examining the beliefs, not the historical behavior, causing emotional turmoil, he could help a patient with their sustained emotional reactions. Aaron Beck developed cognitive therapy (CT) that emphasized interaction between the analyst and the patient to eliminate irrational beliefs and maladaptive thoughts.

The brain. It truly is a thing of beauty. Throughout the course, we examined psychological disorders from multiple angles, but the neuroscience paradigm was by far my favorite. My teacher was doing research on patients with MDD (Major Depressive Disorder). He was specifically examining functional magnetic resonance images (fMRIs), trying to identify the neuropathology behind MDD and to add another level of specificity to the diagnosis and treatment of the disorder. Because of his research done at Stanford, he enjoyed teaching the neuroscience paradigm as well.
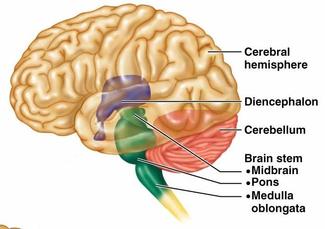
We started with the four major structural areas of the brain: the cerebrum, the diencephalon, the brain stem, and the cerebellum. As part of the cerebrum, the cerebral cortex is the superficial surface of the brain. Because the cerebral cortex is the collection of dendrites at the end of neurons, it is known as gray matter. The creases and folds that make up the brain allow the brain to fit inside the skull. The corpus callosum connects the right and left hemispheres. The insula is an island of gray matter underneath the lateral fissure that is crucial in mood disorders. Finally, the basal ganglia are deep subcortical nuclei important in "gating" (the closing and opening of consciousness ) and repetitive behaviors. The diencephalon contains the brain's "relay station", or the thalamus, and the connection between the nervous and endocrine systems, or the hypothalamus. The brain stem consists of the pons, medulla, and midbrain. The medulla is especially important because it is the center for respiration and circulation. Then there is the cerebellum. This is where motor coordination comes from, giving us the ability to take in sensory and motor inputs.
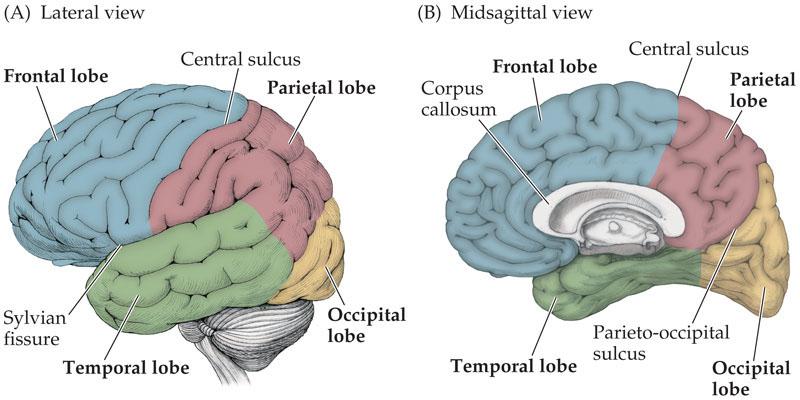
Above is just a picture of some of the brain's major lobes, fissures, sulci, and gyri.
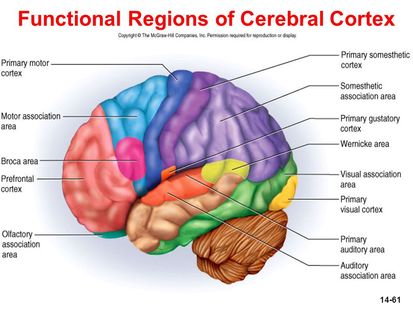
Next, we came upon the functional areas of the brain. It is important to note that functional localization can simply allow people to assess damage done to a brain by looking for functional loss. Above is a picture showing the major functional areas of the brain. Each is the location of some function of the brain. For example, the prefrontal cortex is where higher level functions like abstract thinking and personality come from. My teacher brought of the incident of Phineas Gage who survived a spike through the frontal lobe but lost his personality. The primary motor and somatosensory cortex allow us to execute movement and experience touch. For each primary cortex of one sense is an association cortex that identifies touch, sound, smell, taste, and sight to people, to something of meaning. Language production comes from Broca's area while language reception comes from Wernicke's area. Each function can help identify the location of a certain dysfunction.
This Abnormal Psychology course was particularly interesting because of our professors background in research. For starters, we learned just how amazing PubMed is. I'm addicted. Whenever I hear a TED talk or hear about research, I go to PubMed. My professor taught me how to search the database using my previous knowledge to narrow down the results. Secondly, it allowed our class to work collaboratively. In groups of two or three, we had to write a literature review on a certain mental disorder focusing on a certain paradigm. Our group chose to research Bipolar Disorder and the impact a person's surrounding environment can have on the development and severity of the disorder. Specifically, we researched the effect of childhood maltreatment on Bipolar patients.
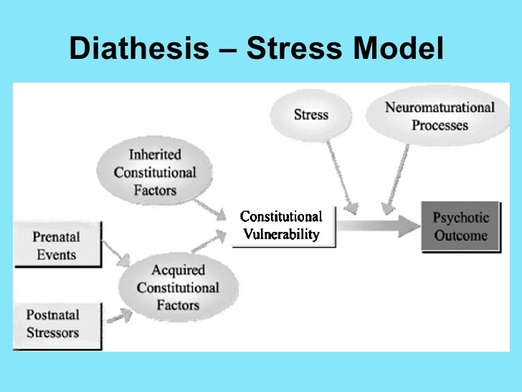
We were inspired to do this research after hearing about the Caspi study. This study found that shorter serotonin transporter genes (homozygous recessive and heterozygous) were more susceptible to depression after exposed to a stressful event. This is known as a diathesis-stress model. "Diathesis" is the biological vulnerability to developing the disorder (like genetics), and "stress" refers to the environmental influences involved. Below is a picture diagramming the diathesis-stress model:
We were inspired to do this research after hearing about the Caspi study. This study found that shorter serotonin transporter genes (homozygous recessive and heterozygous) were more susceptible to depression after exposed to a stressful event. This is known as a diathesis-stress model. "Diathesis" is the biological vulnerability to developing the disorder (like genetics), and "stress" refers to the environmental influences involved. Below is a picture diagramming the diathesis-stress model:

The environment children are raised in do factor into their mental health. In our literature review, we further examined the effects of childhood abuse on the characteristics of the disorder. Us three were the commuter students. We would stay after class as long as we could to work on our paper. Our favorite spot was in the shade under this one tree in the Engineering Quad. We would bask in the sun while reading the papers of Stanford professors themselves. While we did share many laughs, we still challenged each other. I felt I performed significantly better than any other group project I've done because my partners were not afraid to critique my work. They gave me their honest opinion, and I gave them mine. We all shared a love for learning; in our eyes, constructive criticism just helped reveal the true story behind the research (yes, there were many conflicting papers--I was amazed, too).
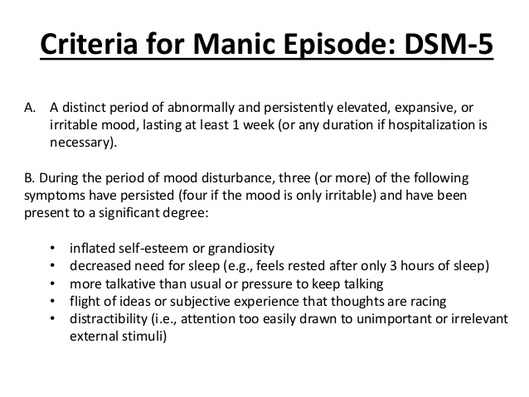
Although it was interesting to research the role of external influences on Bipolar patients, I wanted to know more about the neuroanatomical dysfunctions associated with Bipolar Disorder. People with Bipolar Disorder tend to have overly sensitive receptors. This means an increase in dopamine can lead to manic symptoms. Mania is defined by distinctly elevated and irritated moods with noticeable side-effects. Below I have given the Diagnostic Criteria from DSM-5 of Mania.
Although Bipolar Disorder is less common than a mental disorder like Major Depressive Disorder, it still affects many people, especially in the United States. Not to mention, Bipolar Disorder is comorbid with other horrific anxiety and substance-use disorders. Not to mention, Bipolar patients have a high suicide rate. The age of onset is around the age of 25.
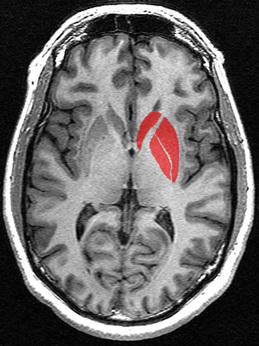
As mentioned before, Bipolar Disorder is the most heritable psychological disorder. Even more significant, Bipolar Disorder correlates with high levels of activation in the striatum during manic episodes. The striatum is where the nucleus accumbens is located. This is the brain's reward system which leads to these elevated moods in manic episodes.
As mentioned before, Bipolar Disorder is the most heritable psychological disorder. Even more significant, Bipolar Disorder correlates with high levels of activation in the striatum during manic episodes. The striatum is where the nucleus accumbens is located. This is the brain's reward system which leads to these elevated moods in manic episodes.
Although my group focused on Bipolar Disorder, our class primarily studied Major Depressive Disorder (MDD). While Bipolar Disorder is much more heritable, MDD is one of the most common psychological disorders. Specifically, many students my age suffer from MDD. In fact, several kids in our class shared their personal experiences with MDD. Just by hearing the stories from your peers makes the material so relatable and therefore powerful. As mentioned before, our professor has done extensive research on MDD. Let's just say there was no one who could have taught it better. We started with the diagnostic criteria:
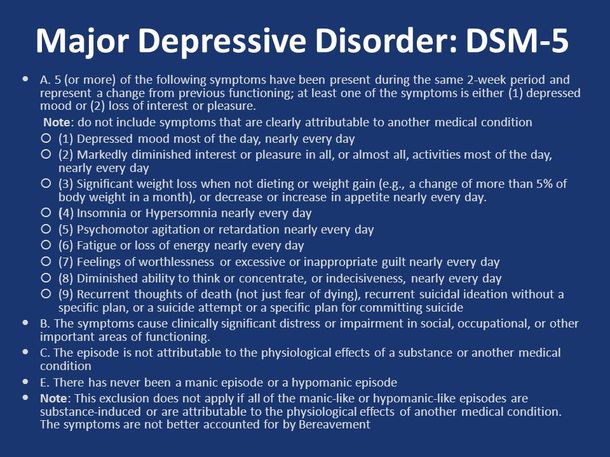
MDD has a high lifetime prevalence of 16.6% (30 million people). It is the leading cause of disability, accounting for 10.8 million DALYs (Disability Adjusted Life Years). Not to mention, it is the most economically burdensome disease. To make it even closer to home, the median age of MDD is teens to 20s.
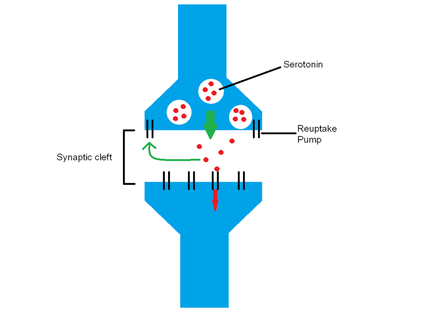
MDD obviously has an impact on all of our lives some way or another. We started by looking at the neurotransmitter findings on MDD. The disorder is notorious for low levels of serotonin and dopamine. Serotonin is produced in the raphe nucleus in the medulla and has major routes throughout the dorsolateral prefrontal cortex. Its route to the nucleus accumbens creates our own psychological reward system. This reward system is deficient in MDD patients. Dopamine is produced in the substantia nigra, and it is responsible for pleasure, motivation, and energy. Dopamine also runs through the nucleus accumbens, but it also goes to the striatum and frontal regions. Some of the most common medications for MDD and other psychological disorders are SSRIs (Selective Serotonin Reuptake Inhibitors). During synaptic transmission, the neurotransmitters travel from the axon terminal of one neuron to the dendrites of another. However, not all neurotransmitters bind to their specific receptors. These neurotransmitters are taken back by the axon terminal of the neuron they came from. SSRIs prevent the reuptake of serotonin to increase levels of serotonin in the synaptic cleft.
MDD obviously has an impact on all of our lives some way or another. We started by looking at the neurotransmitter findings on MDD. The disorder is notorious for low levels of serotonin and dopamine. Serotonin is produced in the raphe nucleus in the medulla and has major routes throughout the dorsolateral prefrontal cortex. Its route to the nucleus accumbens creates our own psychological reward system. This reward system is deficient in MDD patients. Dopamine is produced in the substantia nigra, and it is responsible for pleasure, motivation, and energy. Dopamine also runs through the nucleus accumbens, but it also goes to the striatum and frontal regions. Some of the most common medications for MDD and other psychological disorders are SSRIs (Selective Serotonin Reuptake Inhibitors). During synaptic transmission, the neurotransmitters travel from the axon terminal of one neuron to the dendrites of another. However, not all neurotransmitters bind to their specific receptors. These neurotransmitters are taken back by the axon terminal of the neuron they came from. SSRIs prevent the reuptake of serotonin to increase levels of serotonin in the synaptic cleft.
There are two broad networks in the brain: the Default Mode Network and the Task Positive or Dorsal Attention Network. The Default Mode Network is rumination. This is self-referential processing, or in simple terms, dwelling negatively on insignificant events. The Task Positive Network is all externally motivated activities. People with MDD are stuck in the Default Mode Network due to their highly activated subgenual anterior cingulate cortex (sgACC). The Frontocingulate Network is in charge of affective processing; it regulates the Default Mode Network. In general, frontal regions regulate other regions. For example, the dorsolateral prefrontal cortex (dlPFC) regulates the activity of the sgACC. The sgACC is greatly activated in MDD patients and the dlPFC is barely activated when MDD patients are exposed to a negative stimulus.
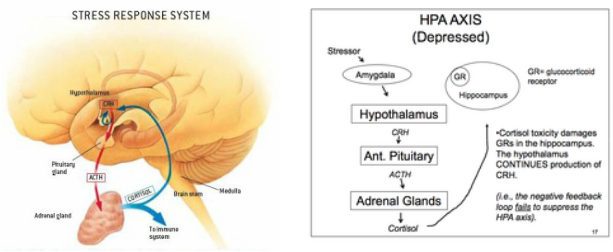
Finally, we came to the hypothalamic-pituitary-adrenocortical axis (HPA axis). The amygdala, which is responsible for our emotional reactions to certain stimuli, is overactive in MDD patients. It triggers the HPA axis to release cortisol, which is the main stress hormone. Cortisol increases activity in the immune system to help the body prepare for a threat. Using Cushing's syndrome (over-secretion of cortisol) as evidence, we know there is a link between high cortisol levels and MDD. In MDD patients, the HPA axis is more sensitive and is poorly regulated, causing people to feel abnormal amounts of stress. The hippocampus of MDD patients is small due to the excess of cortisol.
Finally, we came to the hypothalamic-pituitary-adrenocortical axis (HPA axis). The amygdala, which is responsible for our emotional reactions to certain stimuli, is overactive in MDD patients. It triggers the HPA axis to release cortisol, which is the main stress hormone. Cortisol increases activity in the immune system to help the body prepare for a threat. Using Cushing's syndrome (over-secretion of cortisol) as evidence, we know there is a link between high cortisol levels and MDD. In MDD patients, the HPA axis is more sensitive and is poorly regulated, causing people to feel abnormal amounts of stress. The hippocampus of MDD patients is small due to the excess of cortisol.
On Saturday August 13th, I took my Abnormal Psychology final. I mean the fact that I took a three hour test in a lecture hall next to the room that housed the Stanford Prison Experiment is pretty cool. On one of my rides on the train, I listened to a TED Talk titled "Older People are Happier". I approached my professor about the presentation, and believe it or not, his office was two doors down from the speaker. Before I knew it, I was in the speaker's office, deep in conversation about the beautiful parts of aging and our bodies' biological clocks. That's why I loved this program. There was always a surprise, whether in the material I studied, the people I met, or the places I found on my runs around campus. That final day, as I was taking my last walk through the towering trees and Spanish tiled buildings, I found the Stanford marching band. With only three weeks left until the Stanford football team's first game, I figured they were just rehearsing. However, as I followed the sound, I soon found the marching band playing loud and proud in swimsuits in the fountain in front of the bookstore. I was speechless. I loved how everyone felt free to be themselves, to be a little unique. All the students loved to learn, including the starting point guard for the basketball team (who was in my class). While I loved the class I took, the people were the best part about the program. I found a crowd who worked hard while caring for the people around them. They loved to hear your stories, and they loved to share theirs. They laughed at your jokes, and they told even funnier ones. They definitely were my people.
